
Managing Chronic Osteoarthritis? It is as easy as A,B,C
Stuart Carmichael
BVMS MVM DSAO MRCVS
Fitzpatrick Referrals; UK
Introduction
Osteoarthritis is the most common cause of chronic pain in dogs with estimates indicating that 20% of the dog population is affected by the disease 1. It is also a very common reason for euthanasia in older animals. Fortunately not all animals with pathological changes will show overt clinical signs and those that do can often be successfully managed. Multimodal management has become a popular way and successful way to address the complex global requirements often present in the chronic OA patient with attendance to pain management, nutrition and exercise. But it can be difficult to plan, implement and sustain this program. This is where A,B,C plus D, E and F can be useful !
Pain and Osteoarthritis
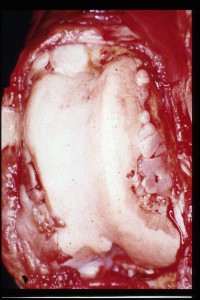
Osteoarthritis is often described as progressive degenerative condition arising within articular cartilage and eventually involving all of the structures in and around the joint (Fig 1). Degradation of cartilage is a progressive process and in time the joint may become unable to function as a result of cartilage destruction and other articular damage. However clinical problems that appear throughout this time are usually the direct result of pain, initiated by the joint pathology. Therefore most of our attempts at managing this disease are aimed at achieving pain control.
At the present time there is no clear method of reversing the pathological process and thus this remains insidiously progressive over a prolonged time interval. This paints a pretty hopeless situation and management attempts often reflect this attitude. Of direct significance to the clinician is the fact that there is very poor correlation seen between both radiographic and pathological state of the problem (Figs 1, 2) and the extent of pain experienced 2,3. Clearly individuals who have advanced changes are more likely to experience pain but the amount and extent cannot be derived from these alone. However many patients with obvious pathology can become and remain clinically improved over sustained periods of time giving more hope and reason for a more thoughtful management effort. There is growing evidence that many dogs with osteoarthritis may be in a chronic pain state4. This is much harder to identify and control than acute pain response in both animals and humans and requires more sustained and longer term analgesia to achieve improvement. Acceptance of the importance of pain in the disease coupled with an understanding that management is really for life have fundamentally shifted the principles for managing the chronic OA patient
Principles for Management
 Chronic osteoarthritis is a complex disease that affects and involves multiple systems rather than just the joint alone. Traditionally the management of osteoarthritis has been focused on the pathological process within the affected joint, and especially on degrading cartilage. To this end surgical alteration and medical intervention aimed at local anti-inflammatory control and chondroprotection have been the main goals of treatment. In a chronic disease process, like the one that we encounter in osteoarthritis, we also must look beyond the target organ and try to understand the way the pain experience is processed and, importantly, how it may be modified to the benefit of the patient. One of the accepted wisdoms in chronic disease is that the pain experience has no protective effect, contrary to acute pain, and is part of the debilitating nature of the disease. So pain plays no positive part in chronic osteoarthritis. By its very nature osteoarthritis is a disease that once initiated persists for the lifespan of the affected patient. As such, all control strategies must take account of this need for long-term treatment. Therefore the objectives for management can be summarised as follows
Chronic osteoarthritis is a complex disease that affects and involves multiple systems rather than just the joint alone. Traditionally the management of osteoarthritis has been focused on the pathological process within the affected joint, and especially on degrading cartilage. To this end surgical alteration and medical intervention aimed at local anti-inflammatory control and chondroprotection have been the main goals of treatment. In a chronic disease process, like the one that we encounter in osteoarthritis, we also must look beyond the target organ and try to understand the way the pain experience is processed and, importantly, how it may be modified to the benefit of the patient. One of the accepted wisdoms in chronic disease is that the pain experience has no protective effect, contrary to acute pain, and is part of the debilitating nature of the disease. So pain plays no positive part in chronic osteoarthritis. By its very nature osteoarthritis is a disease that once initiated persists for the lifespan of the affected patient. As such, all control strategies must take account of this need for long-term treatment. Therefore the objectives for management can be summarised as follows
- Need a strategy that will endure for the life of the patient
- Pain control and elimination is key
- Modification of pain response outside the joint will benefit management
- Sustaining mobility of both joint and patient is essential for a reasonable lifestyle
This does not remove the need or desire to achieve modification of cartilage pathology but rather places it in a more realistic perspective in relation to individual patient management requirements.
Multimodal Management for Osteoarthritis
Achieving satisfactory pain control and maintaining it in the chronic arthritic patient has been shown to be more effective with a more global approach to management than using a single analgesic or anti-inflammatory medical agent 5. A multimodal approach involves targeting a number of different intervention modes simultaneously to achieve more effective control as quickly as possible, and then to modify these as the disease progresses or the patients needs change throughout life6. It involves therapeutic options, which are neither medical or surgical. Obviously an intervention like this requires careful planning and prioritisation. There are different ways in which this can be established to give a logical approach. Fox 7 has identified six key interventions, all of which are based on evidence of positive effect and can be combined to produce synergism when assembled as a multimodal plan. These are identified in Table 1
Table 1 Multimodal Therapy suggested by Fox (2010)7
|
|
|
|
|
|
Evidence of proven benefit is critical given the wide range of choices in this field and the difficulties of assessing benefit from intervention.
This article outlines a similar method but based on different domains for intervention rather than the specific recipe provided by Fox. This is the 6-point plan (AimOA© System) with six different areas for intervention to form a multimodal approach to any arthritis case. (Table 2).
Table 2 AimOA© Multimodal System for OA Management
| A | Analgesia | NSAIDs; Adjunctive Analgesics |
| B | Bodyweight and diet | Obesity control; EPA Diet |
| C | Care | Toxicity monitoring; Practical changes |
| D | Disease | Chondroprotection; Surgery |
| E | Exercise and Rehabilitation | Physical Rehab |
| F | Follow-up | Next appointment |
Using different domains gives more flexibility but still allows a targeted multimodal approach to be followed. It also allows the therapy to be altered through the progress of the disease to better meet the patients needs.
Compliance is essential for this approach to an arthritis problem and the owner must both understand the objectives and be willing to show patience and commitment to achieve benefit. Regular reassessments and recording results to ensure improvement are a must with a system like this
Planning Osteoarthritis Management
One of the main problem in arthritis management is processing all of the choices available and making a selection of an appropriate agent to meet the objectives for treatment. Many attempts at management are based around a single drug strategy. This contradicts the evidence supporting the effectiveness of a multimodal approach suggested previously.
The whole process of managing osteoarthritis can be summarised as follows
- Identification of a problem
- Assessment
- Review possibilities and select intervention strategy
- Assess success of this within a set time frame
- Continue, modify, replace or add to intervention (s)
- Re-assess etc (maintenance phase)
The process must be simple to use, successful in achieving rapid success, sustainable over long term and must bring the clinical problem under the control of all concerned. It must also be practical and economically feasible.
One way of ensuring that there is a controlled approach to the problem is by using pre-determined management plans, which are customised for each patient. These have the multimodal approach imbedded but require judgements to be made about priorities and sequences of treatments used. They combine pharmacological and non-pharmacological methods and will evolve to meet changing needs in dealing with the chronic disease process. This last point provides sustainability.
Successful plans depend on good clinical assessments being made at different times during the management process. These must be repeatable and allow comparison, not only with the last assessment but also with all assessments recorded. This is the key to exerting control over chronic evolving disease processes. Records must be reliable and assessment simple but also accurate at detecting variations in the clinical state. Assessment of a complex disease like osteoarthritis is not an easy feat and is by necessity largely subjective 8,9. Many attempts have been made to construct a scale that can be used to give repeatable measurements of pain with limited success. Carefully constructed client questionnaires may be the most useful way of judging the subtle changes that can indicate early improvement or deterioration 10,11
Maintenance and Management Plans
A critical way in which the approach to the patient with osteoarthritis can be improved is to develop a maintenance approach and include it in the plans. In these situations regular visits at set times are arranged for the animal to be checked rather waiting for the animal being presented when a problem occurs. These are initiated once the initial presenting signs are brought under control and the plan evolves to concentrate on the long-term management issues. This approach is particularly useful in chronic disease where regular assessments can be used to map gradual improvements. It can also allow early identification of developing problems allowing rapid adjustment of plan to preclude serious deterioration. The approach is particularly useful in ensuring that non-pharmacological measures are being maintained and optimised. In many cases veterinary nurses can manage a large component of the maintenance phase through specialised support clinics for arthritic patients.
Proposed Management Strategy for Osteoarthritis
The Six Point Plan for OA Management (AimOA© System) is proposed to satisfy the requirements outlined above. The plan identifies six separate areas of management or modes, which can be addressed simultaneously to deliver a multimodal approach. These areas are identified by alphabetic prompts A, B, C, D, E, F (Analgesia; Bodyweight and Diet; Care; Disease Exercise and Rehab and Follow –up) (Table 2) and presents them as a working plan (Table 3).
Mode A- Analgesia
This is a key mode is any approach to management as most animals will present because they are suffering pain. Medical agents, which have the advantage of producing a rapid alleviation, can achieve pain control. Agents most commonly used for this purpose are the non-steroidal anti-inflammatory agents. There is a good range available for use in the dog and newer additions to the market have increased options for use 12. Analgesia can be augmented in a multimodal fashion by the use of adjunctive analgesics like tramadol, the synthetic codeine analogue 13,14, amantidine 15 and gabapentin . Acupuncture has also been used successfully in arthritic cases16
Mode B – Bodyweight and Diet
The presence of obesity (Fig 3) is a key target in the management of the disease. There is convincing evidence that controlling bodyweight has a major influence of clinical improvement17,18,19,. Adipose tissue itself may not be biochemically inactive and has been implicated as a possible inflammatory influence through the action of leptin 20. Various nutraceutical agents can be considered in this domain. There is increasing evidence that the addition of an EPA rich diet can have a positive influence on the clinical disease 21,22,23. Special diets formulated with EPA are the easiest way to make this adjustment. All dietary interventions will take a period of time to become effective, EPA for instance, will take 4 weeks before any benefit is seen and this must be considered in the timing and evaluation process.
Mode C – Care and Comfort
In this domain care applies to being vigilant about intercurrent disease, especially in older patients. Pre-management blood screening may be indicated here especially if medical agents like NSAIDs are going to be used. Monitoring for any toxicity or problems through the management phase is planned in this domain.
The other factors considered here are those of common sense measures to enhance comfort and environmental modifications such as provision of mats on slippery floors or ramps to help getting animals in and out of cars.
Mode D – Disease Modification and Joint Mobility
Although much of our clinical attention is focused on pain control especially in the early or stages of the disease, methods of altering the disease process and pathological changes within the joint must be considered to preserve the function of the joint or the limb. Surgical interventions including joint replacement or modification can be planned here. Medical agents, which influence or modify the structural disease, can also be added in this domain. However there is scant evidence at the present time for measurable disease-modifying effects as a result of therapeutic use 24. Use of polysulphated glycosaminoglycans and intra-articular visco-substitution with hyaluronic acid may be planned here. Other intra-articular techniques such as stem cell and autologous conditioned plasma can be introduced into the plan in this domain. Controlling and protecting mobility of the joints and ensuring protective muscle function are key to any successful arthritis management programme. These counteract the effects of progressive fibrosis and stiffness in affected joints, which are being poorly used. Various physiotherapy modalities can be employed here to assist the process of physical mobilisation essential to continued pain free joint function
Mode E – Exercise and Rehabilitation
Great advances are being made in this area and planning here can accelerate recovery and prolong function. This can be as simple as giving precise instruction for controlled exercise (Exercise chart) or could involve sharing care with a rehabilitation specialist. This phase is of key importance in the maintenance phase of disease management promoting cardiac fitness in addition to general exercise capability. Planning and using a multimodal approach ensures that measures in this domain still complement and are part of the whole approach.
Mode F – Follow –Up
Planning follow-up visits, which allow re-assesment and re-adjustment of the plan are as important as all of the individual interventions. The focus of the plan will need to change with time as the needs of the animal and challenges presented by the disease alter.
Prioritising and Sequencing Management
When setting the first plan certain modes should be identified as a priority depending on the presentation and stage of the disease. The targets for treatment in different phases of the disease progression or recovery can be identified as follows
- Phase 1 – Obvious Pain and/or Obesity
- Phase 2 – Chronic Pain and Joint Mobility
- Phase 3 – Exercise capability and general well-being
These phases track the course of the disease from acute needs (Phase 1) to maintenance objectives (Phase 3)
The plan simplifies the process by providing options in each area and tracking these over time (Table 3). Each plan should be supported by the use of customised diet sheets, bodyweight monitoring or body score records and exercise charts to facilitate communication. Pre-prepared exercise or rehabilitation charts with a number of different levels of exercise clearly explained are a great time saver and will improve compliance with these plans. The key features of an approach like this can be listed as follows
- It allows a multimodal plan to be set-up and implemented very easily
- All of the practice members are working from the same strategy
- Different members of the team may have different roles to play
- The owner can be informed and instructed easily
- Evolution of care progresses with the changing disease requirements
- Complex problems can be managed by extending into the secondary or tertiary options identified for each problem whilst still following the strategy. These may be non-responsive cases or cases with intercurrent disease (hepatic, renal etc)
- It allows incorporation of new developments as they occur without altering the basic planning process
Assessment sheets (Table 3) will be analysed to give a specific and global view of progress over time. In this way a highly focused and sophisticated plan can be used and maintained with the minimum of effort but to the maximum benefit of the affected animal and owner.
Best practice can be easily delivered within realistic financial targets.
Table 3 Sample Maintenance Plan and Record
| Mode | First Visit | Second Visit (28d) | Third Visit (+28d) etc | |
A |
Analgesia |
NSAID started at maintenance dose | NSAID continued | NSAID continued |
| B | Bodyweight and Diet | Body Condition Score 5Diet Planning– or BCS 3
introduce EPA Diet |
BCS 4Diet continuedAquatherapy?
Continue EPA |
BCS 3Maintenance diet(EPA introduced)
As before |
| C | Care(Screening,Comfort, Common Sense) | Bloods normalUrine normal
Environmental Modification ? Bedding / Car Ramp |
Plan future monitoringMats for floor
Other modifications
|
Establish health monitoring regime
Other ? |
| D | Disease | Radiography ? Evaluate any surgical optionsConsider intra-articular therapy if appropriate | Mobilisation started if pain under control | Continue to improve mobilisation with joint exercises |
| E | Exercise and Rehab | Exercise chart position 5Warm up exercises | Exercise chart position 4Passive mobilisation(Aquatherapy) | Exercise Chart P 2Activity Monitors
Rehab plan |
| F | Follow-up | Phone in 7dCheck in 28d | Check in 28d | Check in 3m |
This allows complex plans to be constructed, which may be necessary in the management of ongoing complex cases
Conclusions
Osteoarthritis is a very complex disease process and as a result presents genuine challenges for management in practices. At present there is not one simple single answer to this problem. Current management advances are being driven by new understanding of the disease and the identification of new tools to control the problem.
Focusing on pain management and developing multimodular programmes that can evolve with the disease problems offer the best chance of successfully managing the clinical problems of chronic osteoarthritis at the present time.
References
- Johnson JA, Austin C, Breuer GJ et al. Incidence of canine appendicular musculoskeletal disorders in 16 veterinary teaching hospitals from 1980-1989 VCOT 1994 7; 56-69
- Dieppe PA, Cushnaghan J, Shepstone L The Bristol OA500 study progression of osteoarthritis (OA) over 3 years and the relationship between clinical and radiographic features at the knee joint. Osteoarthritis and Cartilage: 1997: 5; 87-97
- Gordon WJ, Conzemius MG, Riedesel E, et al. The relationship between limb function and radiographic osteoarthrosis in dogs with stifle osteoarthrosis. Vet Surg 2003;32:451–454.
- Fox SM. Pathophysiology of Osteoarthritic Pain. In; Fox SM, Chronic Pain in Small Animal Medicine. 1st ed. London: Manson Publishing Ltd; 2010 p74-96.
- Grainger R. and Cicuttini F.M, . Medical management of osteoarthritis of the knee and hip joints. MJA, 2004 180 232- 236
- Carmichael S.. Putting theory into practice-best practice management for osteoarthritis. EJCAP (2006) 16: 27-31
- Fox SM. Multimodal Management of Canine Osteoarthritis . In; Fox SM, Chronic Pain in Small Animal Medicine. 1st ed. London: Manson Publishing Ltd; 2010 p189-201
- Waxman AS, Robinson DA, Evans RB, et al. Relationship between objective and subjective assessment of limb function in normal dogs with an experimentally induced lameness. Vet Surg 2008;37:241–246.
- Quinn MM, Keuler NS, Lu Y, et al. Evaluation of agreement between numerical rating scales, visual analogue scoring scales, and force plate gait analysis in dogs. Vet Surg 2007;36:360–367
- Brown DC, Boston RC, Coyne JC et al. Ability of the Canine Brief Pain Inventory to detect response to treatment in dogs with osteoarthritis. J Am Vet Med Assoc. 2008; 233: 1278–1283.
- Wiseman-Orr ML, Scott EM, Reid J, et al. Validation of a structured questionnaire as an instrument to measure chronic pain in dogs on the basis of effects on health-related quality of life. AmJ Vet Res 2006;67:1826–1836.
- Carmichael S. Clinical use of non-steroidal anti-inflammatory agents (NSAIDs); The current position. EJCAP (2011); 21: 1-7
- Kukanich B, Papich MG. . Pharmokinetics of tramadol and the metabolite O-desmethyltramadol in dogs. J Vet Pharmacol Ther 2004; 27: 239-246
- Fox SM. Pharmacologics (Drug Classes). In; Fox SM, Chronic Pain in Small Animal Medicine. 1st ed. London: Manson Publishing Ltd; 2010 p113-137.
- Lascelles BD, Gaynor JS et al . Amantidine in a multimodal analgesic regimen for the alleviation of refeactory osteoarthritis pain in dogs. J Vet Intern Med (2008) 22: 53-59
- White A, Foster N, et al. The effectiveness of acupuncture for osteoarthritis of the knee-a systematic review. Acupuncture in Medicine 2006; 24(Suppl): S40-48.
- Impellizeri JA, Tetrick MA, Muir P. Effect of weight reduction on clinical signs of lameness in dogs with hip osteoarthritis. J Am Vet Med Assoc 2000;216:1089–1091.
- Marshall WG, Mullen D, DeMeyer G, Baert K, Carmichael S The effect of weight loss on lameness in obese dogs with osteoarthritis. Veterinary Research Communications 2010; 34: 241-153
- Marshall W. M., Bockstahler B, Hulse D et al Osteoarthritis and obesity – a review: current understanding of their relationship and the benefit of obesity treatment and prevention in the dog Veterinary and Comparative Orthopaedics and Traumatology 2009; 22: 339-345
- Simopoulou T et al Differential expression of leptin and leptin’s receptor isoform (Ob-Rb) mRNA between advanced and minimally affected osteoarthritic cartilage; effect on cartilage metabolism. Osteoarthritis Cartilage (2007) 15, 872-883
- Goldberg RJ, Katz J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain 2007;129:210–223.
- Roush JK, Dodd CE, Fritsch DA et al. Multicenter veterinary practice assessment of the effects of omega-3 fatty acids on osteoarthritis in dogs. J Am Vet Med Assoc 2010; 236: 59-66
- Roush JK, Cross AR, Renberg WC et al. Evaluation of the effects of dietary supplementation with fish oil omega-3 fatty acids on weight bearing in dogs with osteoarthritis. J Am Vet Med Assoc 2010; 236: 67-73
- Wandel S, Juni P, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ; 2010: 341:c4675
Further Reading
Fox SM, Millis D (Eds). Multimodal Management of Canine Osteoarthritis. Ist edition. London; Manson Publishing Ltd; 2010 .
Fox SM, Chronic Pain in Small Animal Medicine. 1st ed. London: Manson Publishing Ltd; 2010
Need more information
www. ivapm.org (International Academy of Pain Management)